fix a cavity or a broken tooth? If you have you probably were thinking to yourself, what the heck is that? Inlays and onlays are usually prescribed when you have a large cavity or are missing a large portion of your tooth and need a more resilient material. In these situations resin or amalgam fillings wouldn’t do the trick because they would not be able to hold up over time against the force of your bite. Inlays and onlays solve the problem of needing more strength in a restoration without having to take the next step towards a crown.
Inlays and onlays can be performed in one visit with the use of Cerec technology. Cerec allows you to fabricate a custom restoration out of porcelain outside of the mouth. This restoration is then cemented into place. It used to be that in order to do an inlay or onlay you need to prepare the tooth, take an impression, send that to a lab, wait 2-3 weeks with a temporary in your tooth, and THEN come back and cement the permanent restoration into place. With Cerec technology you can leave the office with a custom made restoration permanently cemented into place in one visit. It eliminates the need to deal with impression material, the wait until you get your final restoration, or the worry that you will lose your temporary filling why you are waiting all that time.]]>
the force of your bite. Inlays and onlays solve the problem of needing more strength in a restoration without having to take the next step towards a crown.
Inlays and onlays can be performed in one visit with the use of Cerec technology. Cerec allows you to fabricate a custom restoration out of porcelain outside of the mouth. This restoration is then cemented into place. It used to be that in order to do an inlay or onlay you need to prepare the tooth, take an impression, send that to a lab, wait 2-3 weeks with a temporary in your tooth, and THEN come back and cement the permanent restoration into place. With Cerec technology you can leave the office with a custom made restoration permanently cemented into place in one visit. It eliminates the need to deal with impression material, the wait until you get your final restoration, or the worry that you will lose your temporary filling why you are waiting all that time.]]>
 completed but some of the great smiles we noticed along the way!
Top 5
#5 Serena Williams, a dominating performance in the women tennis final, and a beautiful smile to go along with it.
#4 Allyson Felix, the long-time star finally reeled the gold in the 200 m. It was nice to see someone with such nice pearly whites beaming from ear to ear.
#3 Dana Vollmer, Wow! Three gold medals and one of the top smiles in the Olympic games.
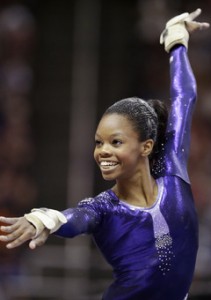
#2 Gabby Douglas winner of two gold medals, who’s smile is literally contagious.
Our top pick for biggest and brightest smile is winner of Five Olympic medals, four gold and one bronze, Missy Franklin (who recently had her braces removed)
A couple of side notes:
Honorable mentions going to our Olympian braces wearer Lashinda Demus and a nod to Ryan Lochte for his patriotic grill.
Finally, Congrats to Michael Phelps for achieving what no other Olympian has ever done. However, we would love to see him straighten out that well known smile with invisalign or braces one day.
Go USA!]]>
completed but some of the great smiles we noticed along the way!
Top 5
#5 Serena Williams, a dominating performance in the women tennis final, and a beautiful smile to go along with it.
#4 Allyson Felix, the long-time star finally reeled the gold in the 200 m. It was nice to see someone with such nice pearly whites beaming from ear to ear.
#3 Dana Vollmer, Wow! Three gold medals and one of the top smiles in the Olympic games.
#2 Gabby Douglas winner of two gold medals, who’s smile is literally contagious.
Our top pick for biggest and brightest smile is winner of Five Olympic medals, four gold and one bronze, Missy Franklin (who recently had her braces removed)
A couple of side notes:
Honorable mentions going to our Olympian braces wearer Lashinda Demus and a nod to Ryan Lochte for his patriotic grill.
Finally, Congrats to Michael Phelps for achieving what no other Olympian has ever done. However, we would love to see him straighten out that well known smile with invisalign or braces one day.
Go USA!]]>
 With the increase in painkiller abuse in America there is a lot of speculation as to who is responsible for this epidemic? Is it the patient with the addiction or is it the ease of legal access to these drugs? This has always been a tough subject for health care professionals, especially those in the dental field.
With the increase in painkiller abuse in America there is a lot of speculation as to who is responsible for this epidemic? Is it the patient with the addiction or is it the ease of legal access to these drugs? This has always been a tough subject for health care professionals, especially those in the dental field.
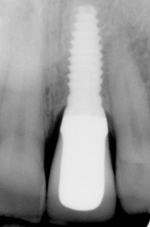 What is the cost of a dental implant? Why is there such a variation in fees for dental implants? Are the advertisements I see for $499 dental implants too good to be true? When trying to figure out what the appropriate fee for a dental implant should be one should know exactly what the procedure entails. Here are the dental implant facts:
What is the cost of a dental implant? Why is there such a variation in fees for dental implants? Are the advertisements I see for $499 dental implants too good to be true? When trying to figure out what the appropriate fee for a dental implant should be one should know exactly what the procedure entails. Here are the dental implant facts:
- There are about three parts that make up an implant restored tooth. The implant, which is surgically placed into the jaw and acts as the root. The post, which screws into the implant to connect the implant to the crown. Then finally the crown, which is cemented or screwed onto the post.
- To have an implant placed and completed start to finish can take between 3-6 months. However with each person the timeline may vary. Time can be added to this treatment if the area needs to have bone grafting. Bone grafting helps regenerate missing bone in areas where there is not enough space for an implant. This can add about 3-6 months to your overall procedure timeline as the grafting is normally done before the implant surgery.
If you’ve been following the news recently you may have seen articles about legislation trying to pass laws allowing increased use of Dental  Therapists in under-served populations. There has been a lot of controversy about this subject because of exactly what a dental therapist is and their role in dental care in the United States.
Currently dental therapists are allowed to practice in Alaska and Minnesota. However, there has been discussion about other states such as Connecticut, Oregon, New Hampshire and California allowing dental therapists to practice. Dental therapists are defined by the University of Minnesota School of Dentistry as ” a licensed oral health professional who practices as part of the dental team to provide educational, clinical and therapeutic patient services. Dental therapists provide basic preventive and restorative treatment to children and adults, and extractions of primary (baby) teeth under the supervision of a dentist. Dental therapists work primarily in settings that serve low-income and under served patients, or in a dental health shortage area.”
Individuals participating in dental therapy programs have training that is significantly shorter than general dentists. A dental therapist must complete at least one year of undergraduate college course work before they can participate in a 2 1/2 year program to teach them the basic skills of local anesthesia, preventative dentistry (such as cleanings and dental sealants), uncomplicated extractions, radiology as well as diagnosis and treatment of cavities. As opposed to general dentists who, in most circumstances, must complete four years of undergraduate college, four years of dental school and in New York state a year of residency.
So what exactly is all the commotion about allowing dental therapists to practice in under served areas? There has been a question about how to address the growing need for care, especially with children, however due to therapists limited training the American Dental Association has brought up concerns that they are not equipped to provide the level of care necessary to complete many of the procedures they are being licensed to perform. And, since many are not reversible such as extractions and fillings, there should be better training of these professionals. Other organizations have made the argument that patients that have medicaid or are in areas with a poor dentist to patient ratio are unable to receive appropriate dental care due to cost of dentistry and many general dentists not accepting these patients into their practices. So the conundrum is how do we provide appropriate care for this needful population in a safe and ethical way. Are dental therapists the solution to this problem or the creation of an even bigger problem?]]>
Therapists in under-served populations. There has been a lot of controversy about this subject because of exactly what a dental therapist is and their role in dental care in the United States.
Currently dental therapists are allowed to practice in Alaska and Minnesota. However, there has been discussion about other states such as Connecticut, Oregon, New Hampshire and California allowing dental therapists to practice. Dental therapists are defined by the University of Minnesota School of Dentistry as ” a licensed oral health professional who practices as part of the dental team to provide educational, clinical and therapeutic patient services. Dental therapists provide basic preventive and restorative treatment to children and adults, and extractions of primary (baby) teeth under the supervision of a dentist. Dental therapists work primarily in settings that serve low-income and under served patients, or in a dental health shortage area.”
Individuals participating in dental therapy programs have training that is significantly shorter than general dentists. A dental therapist must complete at least one year of undergraduate college course work before they can participate in a 2 1/2 year program to teach them the basic skills of local anesthesia, preventative dentistry (such as cleanings and dental sealants), uncomplicated extractions, radiology as well as diagnosis and treatment of cavities. As opposed to general dentists who, in most circumstances, must complete four years of undergraduate college, four years of dental school and in New York state a year of residency.
So what exactly is all the commotion about allowing dental therapists to practice in under served areas? There has been a question about how to address the growing need for care, especially with children, however due to therapists limited training the American Dental Association has brought up concerns that they are not equipped to provide the level of care necessary to complete many of the procedures they are being licensed to perform. And, since many are not reversible such as extractions and fillings, there should be better training of these professionals. Other organizations have made the argument that patients that have medicaid or are in areas with a poor dentist to patient ratio are unable to receive appropriate dental care due to cost of dentistry and many general dentists not accepting these patients into their practices. So the conundrum is how do we provide appropriate care for this needful population in a safe and ethical way. Are dental therapists the solution to this problem or the creation of an even bigger problem?]]>
 The basics:
Generally there are two types of floss: Rope and Tape. They are either waxed or un-waxed.
Tape: a flat string usually made of a smooth material: this is the type of floss that we recommend the most due to the ease of use between tight teeth and teeth with a lot of restorative work such as fillings and crowns.
Rope: this is usually a braided or round string or rope that can be covered in wax or not, depending on your preference. I tend to avoid this type of floss due to the difficulty of use. Often times if you have tightly contacting teeth this type tends to fray or break more often than a tape will.
Specialty floss and floss threaders: There are a series of flosses and floss threaders that are made specifically to be used around bridge work and braces. Super Floss is a brand that I recommend often for patients because it is a thick and spongy floss with a flexible plastic end that is relatively easy to use underneath bridgework and around orthodontic brackets.
Dental Flossers: these are small plastic handles with floss attached at the end, most often a rope type of floss. My opinion on floss threaders is, if you find that you can not or will not use any other type of floss then they can be used. But I rarely recommend them since you lack the ability to maneuver them around the teeth appropriately and can do a little damage to the gums if the patient is not careful when using them.
Water pics and Air flossers: these are electric tools similar to an electric tooth brush that either use air or water to force debris out from in between teeth and out from under restorative work. My opinion on these tools is that while I believe that they have improved water pics and air flossers immensely in the past few years, they are an adjunct to the use of regular floss. The use of regular dental floss is still the gold standard.]]>
The basics:
Generally there are two types of floss: Rope and Tape. They are either waxed or un-waxed.
Tape: a flat string usually made of a smooth material: this is the type of floss that we recommend the most due to the ease of use between tight teeth and teeth with a lot of restorative work such as fillings and crowns.
Rope: this is usually a braided or round string or rope that can be covered in wax or not, depending on your preference. I tend to avoid this type of floss due to the difficulty of use. Often times if you have tightly contacting teeth this type tends to fray or break more often than a tape will.
Specialty floss and floss threaders: There are a series of flosses and floss threaders that are made specifically to be used around bridge work and braces. Super Floss is a brand that I recommend often for patients because it is a thick and spongy floss with a flexible plastic end that is relatively easy to use underneath bridgework and around orthodontic brackets.
Dental Flossers: these are small plastic handles with floss attached at the end, most often a rope type of floss. My opinion on floss threaders is, if you find that you can not or will not use any other type of floss then they can be used. But I rarely recommend them since you lack the ability to maneuver them around the teeth appropriately and can do a little damage to the gums if the patient is not careful when using them.
Water pics and Air flossers: these are electric tools similar to an electric tooth brush that either use air or water to force debris out from in between teeth and out from under restorative work. My opinion on these tools is that while I believe that they have improved water pics and air flossers immensely in the past few years, they are an adjunct to the use of regular floss. The use of regular dental floss is still the gold standard.]]>
Sorry for the brief hiatus or our weekly blog. But, we have some great news!
We would like to welcome the newest addition to the Frangella Dental family!
Introducing, Lea Mary Davis

Lea was born on June 9th at 2:10 pm to Dr. Tina Frangella and her husband Dr. Brian Davis. She weighed 6 pounds 4 ounces and was 20 inches long. Baby and mom are doing great and are recovering at home.
]]> With studies coming out everyday linking how important a healthy lifestyle is its no surprise to see  changes in the diet choices of the general population. Besides overall health nutrition and dental health is also an important subject that many are not aware of. Vegetarians; whether lacto-vegetarians, ova-vegetarians, semi-vegetarians or vegans; as well as people dieting or radically changing their diet, should be more aware of the food they are eating to be sure they are including foods rich in the vitamins and minerals needed to keep your body healthy and your smile beautiful.
Being a dentist we find that we see nutritional deficiencies apparent in the tissues of the mouth before you may notice them elsewhere. Some of the more important nutrients that may be neglected when changing your diet that are important for your oral and general health are:
changes in the diet choices of the general population. Besides overall health nutrition and dental health is also an important subject that many are not aware of. Vegetarians; whether lacto-vegetarians, ova-vegetarians, semi-vegetarians or vegans; as well as people dieting or radically changing their diet, should be more aware of the food they are eating to be sure they are including foods rich in the vitamins and minerals needed to keep your body healthy and your smile beautiful.
Being a dentist we find that we see nutritional deficiencies apparent in the tissues of the mouth before you may notice them elsewhere. Some of the more important nutrients that may be neglected when changing your diet that are important for your oral and general health are:
- Calcium: This nutrient is very important for bone health, as well as helping to maintain healthy gums and reduce your risk for cavities. Calcium is typically found in leafy green vegetables, dairy products, as well as in legumes and some shellfish.
- Vitamin B12 and Vitamin B2: A deficiency in these two vitamins can cause mouth sores. Vitamin B2 can be found in milk and cheese, leafy green vegetables, beans, bananas, and almonds. Vitamin B12 can be found in some shellfish, cheese, and eggs.
- Niacin or Vitamin B3: A deficiency in this vitamin can cause bad breath and sores in the mouth. Niacin can be found in eggs, tuna, salmon and halibut, avocados, dates, leaf vegetables and various nuts and legumes
- Vitamin D: this nutrient helps with the absorption of calcium, when lacking vitamin D some may suffer from something called burning mouth syndrome which can cause and uncomfortable sensation of the tongue and mouth.
- Iron: a decrease in Iron can present itself as a sore inflamed tongue and may cause sores inside your mouth to form as well. Iron-rich foods are eggs, lentils and other dried beans, shrimp, cod and tuna, spinach, sweet potatoes, broccoli and peas. Accordingly foods that boost iron absorption the most are meat, a good iron supplement and foods high in vitamin C.
- Vitamin C: this vitamin is important for healing as well as general health a deficiency can present itself as bleeding gums and loose teeth. You can find vitamin C in Citrus fruits, sweet potatoes and red peppers.
- Some other important vitamins for oral health are Vitamins A, E and K.
Many of our patients know that we consider fluoride an amazing tool. The increased use of fluoride has  changed dentistry radically over the past forty years or so. So although you probably are familiar with fluoride, this post is really to answer the question: Why do I need fluoride? What are the benefits? What are the risks? So lets start with the facts:
changed dentistry radically over the past forty years or so. So although you probably are familiar with fluoride, this post is really to answer the question: Why do I need fluoride? What are the benefits? What are the risks? So lets start with the facts:
Fluoride is a naturally occurring compound found in water, soil and food.
Fortifying drinking water has been recommended by the U.S. Public Health Service to aid in the prevention of tooth decay, they recommend adjusting the naturally occurring fluoride level of existing public and private water sources to reach the optimal level of fluoride which is 0.7-1.2 parts per million or milligram per liter. Fluoride helps prevent cavities by being absorbed into the enamel of the your teeth and fortifying it, making the enamel more resistant to decay and demineralization. This can help in preventing early weakening in the tooth structure and early decay.What are the risks of using fluoride?
The CDC has done numerous studies, the most common risk noticed is dental fluorosis if fluoride is consumed in a high amount for a long period of time during the development of the adult teeth. Dental fluorosis is pitting or mottling of the enamel of the teeth. Children 8 and younger are the most at risk for dental fluorosis. Also, There has been some speculation about a link between fluoride and osteosarcoma however over the past 60 years of fluoride use and studies no link has been established between bone health and fluoride.- The CDC has listed water fluoridation as one of the 10 greatest public health achievements of the 20th century
- The first city to adjust the level of fluoride in its water supply was Grand Rapids, Michigan on January 25, 1945
- Although not all water supply is fluoridated around 72.4% of the U.S. population receive fluoridated water.
- Aside from fluoridated water you can obtain fluoride from a multitude of sources. Such as, fluoride multivitamins for children, in some foods, as well as many mouth rinses and toothpastes.
- Fluoride is endorsed and recommended by the American Dental Association as well as many other state and local dental societies.